ADHD or Bipolar Disorder: Overlap, red flags, and emotional dysregulation
Jun 01, 2022You probably have heard a little of my story. ;)The mission is to help you understand the unique children in your life and support the kids as they grow into thriving adults - and enjoy the journey on the way. One of the things I do on that mission is help address questions such as:
- "Is it ADHD or [___?___]"
- What does an OT/SLP/etc. do?
- Specific parenting challenges - like overcoming loneliness
You're invited to find topics such as those and others on the ADHD-What Now YouTube channel.In fact, today, I'm introducing Dr. Kennedy of the Brown ADHD Clinic to cover "ADHD or Bipolar Disorder: Overlap, Red flags, and Emotional Dysregulation."Stick around to find the answers you need for your kid and your family!
Links
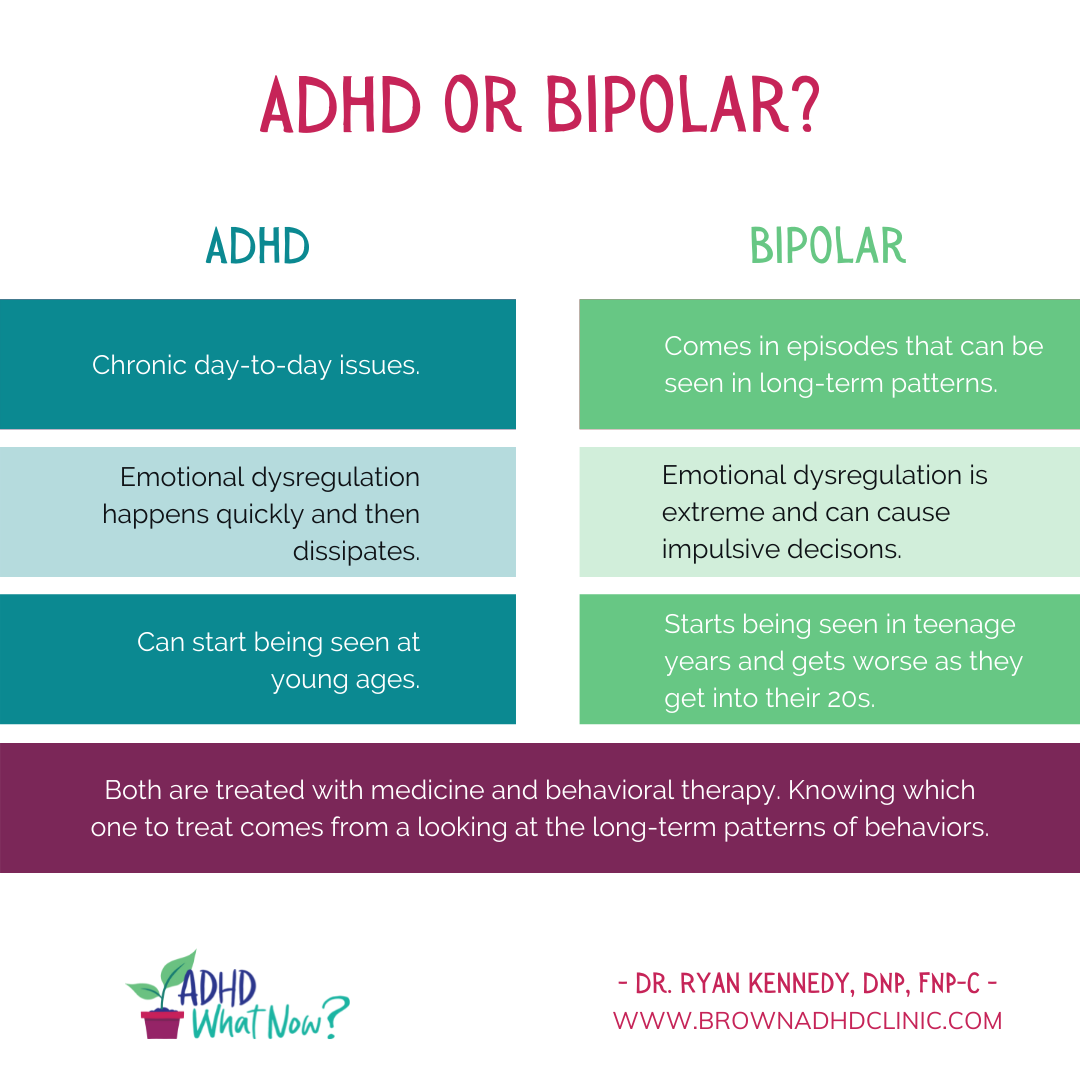
SHAREABLE GRAPHIC
FULL TRANSCRIPT
Veronica: Have you wondered, is it ADHD or bipolar that is going on for your kiddo in your family? My name is Veronica Hunter with ADHD - What Now?, where we cover investigating the body and the brain, growing skills, and building great relationships. And of course, one of the questions that many people have is what support do I get for my kiddo? How do I identify what's going on? And then what support can I get in place?
And so today I'm delighted to welcome Dr. Kennedy of the Brown Clinic, and he is here to address for us, is it ADHD or bipolar, and tease out some ideas around emotional dysregulation for us. So, welcome Dr. Kennedy. It's great to have you here.
Dr. Kennedy: Thank you for inviting me. Hopefully we have a good session and answer some questions that are helpful to some people.
Veronica: Awesome. Now you are part of writing, or wrote, an excellent article in ADDitude magazine that was titled "When a Mood Disorder Looks Like ADHD - and Vice Versa: Differentiating Signs of Emotional Dysregulation". And what I loved about that article was that it added a lot of clarity and just showed how, well you were able to - or help people identify the details of that. So, I'm hoping that throughout this conversation, you'll share a bunch of that too.
So to dive right in, like you have many families that are probably coming to you and asking what is going on. So when we're talking about emotional dysregulation, like, what does that look like? What do they come to you saying?
Dr. Kennedy: So at our clinic, we see little kids, teenagers, and adults who may have ADHD, or they're coming to see us for a second, third, sometimes a fourth opinion, because they are asking for some diagnostic clarity. And they've had treatments in the past, but are not quite successful in alleviating a lot of their difficulties.
And as far as the emotion dysregulation, it's not something that's been put into the diagnostic criteria for ADHD, but it is an associated symptom for some people. But breaking down the emotional dysregulation; some people think that it's separate from ADHD or overlaps with another. And so for our clinic, we are able to see patients for three hours. And during that time, most of it is just asking a million questions in a clinical interview, see an understanding of the person's strengths and difficulties, that family dynamic, and sort of the course of illness. And depending on their age, will steer some of the diagnosis, particularly if we're dealing with kids that are 12 and under, or are likely not to be thinking this is emotion dysregulation with bipolar disorder or a mood disorder, rather ADHD, possibly with anxiety, with a depressive mood, that's just beginning to erupt, or sometimes it's the parenting style between the parents.
Sometimes if the parent doesn't have their own ADHD recognized, you can have this turmoil in the house between, you know, the parents. For adolescents, it gets a little tricky sometimes with puberty where the surge of hormones is starting to happen.
And some people that is just a temporary period of time. And some people would like to think that they're having a worsening ADHD or do I have another disorder. And so in our evaluations, we really get a lot of time to use our rating scales, which are normed and nationally validated. So we can hone in on, is this more poor executive functioning and ADHD, or do we need to have another follow-up assessment? And sometimes we don't know, sometimes with like, for example, bipolar type two, it takes quite awhile to really get enough examples and seeing the person over time to see the patterns. With ADHD, it's much more chronic day-to-day and that is easier to recognize, at least for us in our clinic.
Veronica: So can you describe what is meant by emotional dysregulation, first of all, like, what does that core term mean?
Dr. Kennedy: So there are a few different definitions of it. How it fits with ADHD, it's not my favorite terminology for it because it's has so many other diagnoses associated with it. For example, with personality disorders like borderline personality, emotional dysregulation is almost a guaranteed with that disorder. Where with ADHD, it's a smaller percentage. The range is somewhere between 30 to 70%. And it has a lot to do with temperament, personality, and life circumstance stressors.
So the emotional dysregulation you see with ADHD, it's quick, it's over with, and then people feel, you know, sorry about it. And then, you know, but it happens in this continuous sort of pattern, but it's not something that's sort of extreme and out of nowhere and has the quality of that of other disorders, like where there's a splitting of, "I hate you, you're the worst person in the world," from one day to the next and "you're the best and I love you".
And so you can sort of see how the emotion comes out. A lot of people with ADHD, it's, if it's untreated, it's the chronic frustration, the irritability, the easily discouraged, it's hard to snap out of it. And how you can see that sometimes is we do working memory testing.
And for example, there's all sorts of working memory tests. One we like to use is using stories. So patients, they listen to two short stories, each about 25 units, and as they're listening to it, they're trying to keep it in mind. And then when I stop, I ask them to repeat it back to me. Most patients, whether they're average smarts to very high IQ, tend to do poorly on that test. It's a rough test of working memory, but it tells me something about how well they can keep things in mind while doing something else.
And that is a lot of the core symptoms or the driver behind how the emotion regulation works for them. It's hard for them to snap out of an emotion, it's as if like a computer virus takes over their brain. And once that emotion hits, whether it's discouragement, anxiety, nervousness, or depression, when it happens, it happens fast,
hard, and it's over quickly, usually.
Veronica: For ADHD?
Dr. Kennedy: For ADHD. So it has a sort of quick buildup to it. And then it's over quickly. And for some kids, they can usually hold it together a lot at home, I mean, at school particular for, you know, fear of peer rejection and they don't want to look bad in front of their teachers and have, you know, remarks and get in trouble.
So, some kids when they come home and that's when you see it. But kids who are bipolar, they have more of the impulsiveness that can get a bit extreme and they can get up in fights and arguments at school. So getting an idea of the location of where things are happening helps sort of steer the understanding of it.
Veronica: So how often do they co-occur together, ADHD and bipolar?
Dr. Kennedy: So by statistics, ADHD is more common, has a higher prevalence rate than bipolar disorder. The emphasis on bipolar disorder is usually on bipolar type one; bipolar type two gets missed a lot. So the data for that I think is often under diagnosed.
But for kids and adults, the general consensus for ADHD is somewhere between three and seven to 9%. And the overlap with a bipolar disorder is similar to that same percentage, but tends to be a little bit less. The bipolar two is more sneaky to diagnose, but likely more prevalent than current data suggests.
Veronica: Okay. So looking then, help us understand what is the difference or what can we be aware of as far as ADHD versus bipolar so that we can get to someone such as yourself that will help to tease apart those two things.
Dr. Kennedy: So sometimes if we suspect someone has a bipolar diagnosis, we're going to use validated rating scales in our clinic to determine which is the priority diagnosis or symptoms, because these, you know, symptoms of emotional regulation can overlap between the two. But what else is there with their difficulties that takes priority? If for example, someone has a bipolar type one diagnosis, then stimulants or ADHD treatment is not going to come first and we're going to initiate some treatment plan to support the patient with bipolar one disorder, do a lot of psychoeducation.
And if it's bipolar type two, it doesn't always require bipolar medication, but usually requires some sort of action plan. And that in and of itself is a lot psychoeducation, which if I have to repeat it seven more times, that's essentially the most important part of getting people to really understand their illness and knowing that it can change over time.
For both disorders, they usually run in families. So if someone is coming to see us, you ask good questions and they start to think about people in their family, you'll usually be able to find someone, whether it's their parent or, you know, an uncle or a cousin. Both are equally as heritable and science uses numbers between zero and one to say how likely something to be passed down from the parent to their child. And that scale is zero to one. ADHD is 0.76 and bipolar is about a 0.8.
So most people, for either disorder, you can usually find someone else with it. And that helps give us a clue about which direction we may want to go for treatment. But I've had families where that becomes a bias as well. And because grandpa had, you know, bipolar disorder, without me having to verified that, the parents may have inclination, "oh we need to treat this as bipolar," and we don't get the correct ADHD diagnosis. And sometimes it gets tricky to do this or the unconvincing of, we need to start from scratch here.
But we do have, I like to use pictures and like plenty of explaining sort of the course of symptoms. Like if we're talking about bipolar there's, this was just a drawing example of the highs and lows. And some people may feel like with ADHD that they could fit into this, and sometimes they do. But what we're really looking for is a long-term pattern of behavior and getting feedback from as many people as possible helps to see which diagnosis really is the priority for treatment.
Veronica: Which is important because as you mentioned that the treatment regimen is different depending on the identification of the problem.
Dr. Kennedy: Correct. So we really try to narrow our targets of what the difficulties are. For both, it's usually medicine with behavioral treatment. And particularly if, well, it doesn't particularly matter which diagnosis someone has, but having a family support, friends, anyone in your community who helps understand them so they can see the signs of it.
Say someone has a bipolar diagnosis, nobody knows when they may have an episode, they may only have one. They may have a type that comes once a year. So having someone recognize the early signs of it, then it can be treated. With ADHD, it's more of the day to day thing.
Veronica: Okay. So what does bipolar one look like or mean?
Dr. Kennedy: Bipolar one is just very distinct from type two. It is based on its severity. Most people who have bipolar one, the symptoms are prodromal in they're late teens. And the illness gets worse as they get into their twenties, that's the sort of the typical pattern.
Same for bipolar two. It's rare, very rare to see it in young kids. There's sometimes little signs depending on their temperament style, but generally you see it at their late teen years.
The similarity that both have is their depressive symptoms can be just as bad. And people with bipolar two, they usually stay in that state and then they go to a normal mood. They only need one hypomanic episode in their life to have a diagnosis, but some people would disagree.
What that hypomanic is racing speech, racing thoughts, talk way too much, not needing to sleep for a day or two or three, and then it's over. And it usually doesn't always impact their life. Sometimes these people can be very creative and make wonderful business deals and do a lot of great productive work with all of that energy and not cause any problems in their life, cause chaos.
The other type, type one usually ends up in the hospital because they're unstable, unsafe and they make decisions that are very risky. And sometimes it leads to hurting themselves or getting too much involved in substance use.
Veronica: So for bipolar type two, what are red flags to be aware of?
Dr. Kennedy: So sometimes what you'll see is the buildup of it. It is I have all this energy, I'm not sleeping, you know, three, four days, they get more goal directed behaviors. And if they're in their career or they're an artist, they're spending a lot of time awake doing art work and they could be making very beautiful stuff, there's nothing strange about it.
Just, "Hey, are you getting any sleep?" And then sometimes that shifts to more irritability and then they crash. And this is like three days, four days, maybe up to a week of just sleeping and not wanting to be around society. So there's this hit and peak to the disorder, but it's short lasting. And seeing that happen once may not be enough for some people that say that warrants a assessment.
But when you see it happen, time and time again, and it starts to cause a disruption to maybe the relationship with the people they live with or forgetting to pay bills or something. And that's taking care of day-to-day tasks or losing clients. That's, you know, as people get older, they start to see that, okay, this is more like bipolar two and we need an assessment for it.
So the emotional dysregulation, how that fits within all of it, it can be tricky to separate between the two.
Veronica: So bipolar at school and at home, what does it look like?
Dr. Kennedy: So, I have a young girl, she's in high school and she's an amazing artist. At school she had a lot of trouble connecting with other people because of what she thinks of herself. And no one would know. It's not like she's walking around with a label on her forehead of, "Hey, I have bipolar disorder". But it's the symptoms that she's discussed is that primarily at home. Most people at school she tries to avoid cause they don't, she doesn't want to let them in to see that side of herself.
There was a really great New York times article written in the nineties and I think became a movie starring Anne Hathaway, Take Me As I Am. That's a wonderful story about a woman who's very successful and had two sides of herself. One that everybody knew, who she was very outgoing, she was funny and successful, and everyone wanted to be around her. But then when she would crash as part of her bipolar two phase, she would disappear. No one would know where she was, and then she would come back.
Similar to my patient; she goes through these sort of, she calls them spells. And you can see when she's at her best. And then when she hits these lows, the lows are pretty bad, but she doesn't ever get to that very, very manic phase where we're considering hospitalization.
It's usually a specific medication protocol we have that helps that ramp up, calm down. And it's not something she has to miss school on. It just helps her reduce that level of intensity or energy that she has. So if she were to go to school, no one's going to notice that pressured, you know, fast paced speech, or "gee, you haven't slept in three days". So it helps to regulate her energy level.
Veronica: Awesome. That helps clarify a lot. What other thoughts would you like to leave families with regarding emotional dysregulation, ADHD or bipolar?
Dr. Kennedy: An important takeaway I give to a lot of parents is a philosophy we use here: you catch more flies with honey than vinegar. And that has to do with your spouse or with your kids or how you deal with yourself.
And regardless of your difficulties, you can't just say, okay, I have ADHD, and that explains why these are my problems and I don't deal with them. But do be proactive about your diagnosis, have the right treatment plan.
Sometimes you need a second opinion, learn as much as you can about it and yourself and having your family back you up. I think that that's essential for everybody. The medication is kind of the boring part and in my follow ups I like to learn about how people are functioning. So I ask a lot of questions with parents while they're here or with their kids and try to see just generally how they're doing and when they leave here, hopefully they feel good about themselves.
Veronica: Awesome. Thank you so much for being here today and for sharing about ADHD, and bipolar, emotional dysregulation and what some red flags are, and how to get help, very much appreciate it. And where can people find you online and your practice? How are you accessible?
Dr. Kennedy: Thank you. It was great to be here. The easiest way to get in touch with our office is through our website, BrownADHDclinic.com. And you can visit our website.
If you have an appointment, we have an easy button to click on to self-schedule, or you can just give us a call. If you have questions you can email us. And that email address is right on the front page. It's the [email protected].
Veronica: Awesome. Thank you. And for anybody watching put in down below in the comments, what was useful for you about this conversation and like, subscribe, and I'll see you later.